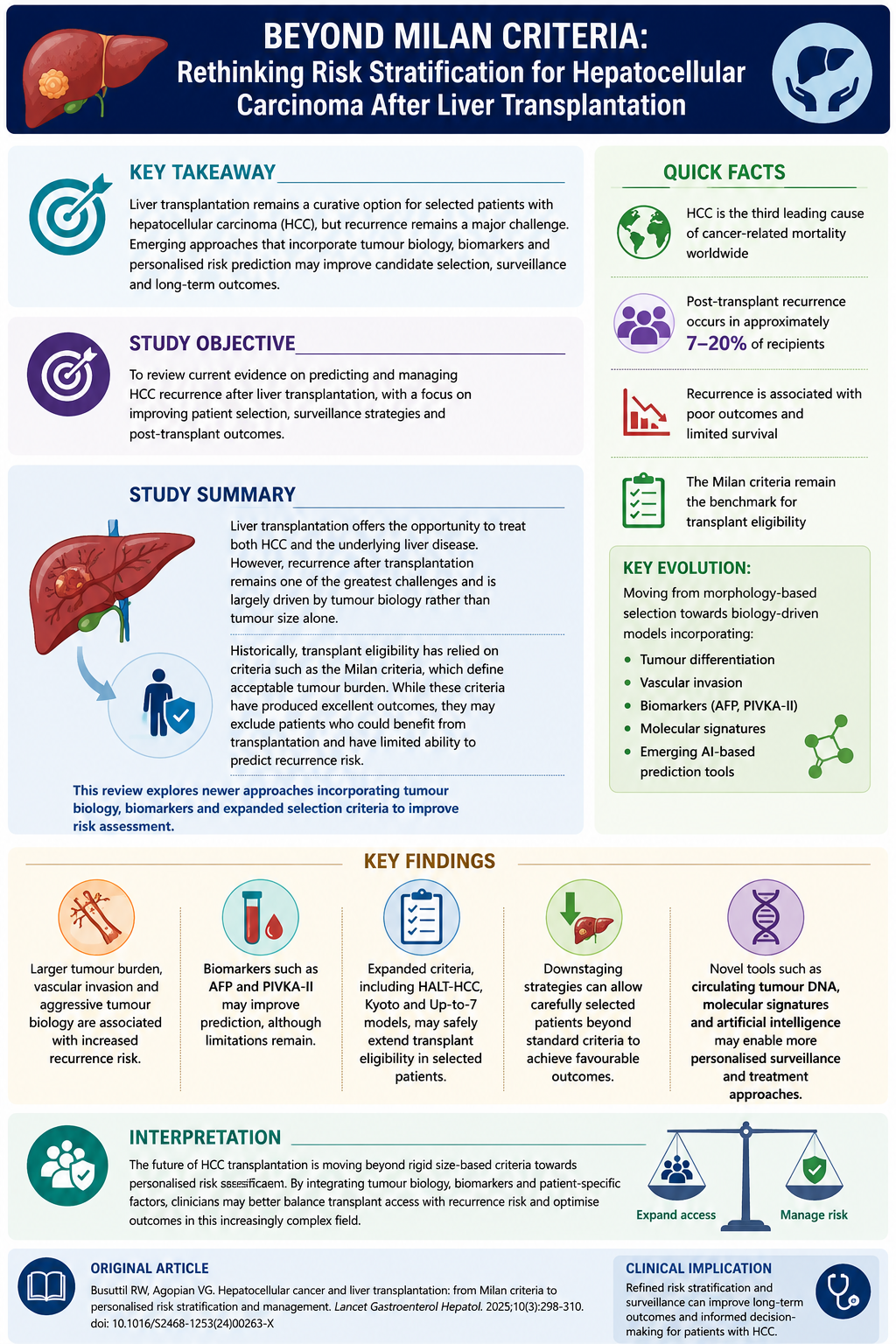
To review current evidence on predicting and managing HCC recurrence after liver transplantation, with a focus on improving patient selection, surveillance strategies and post-transplant outcomes.
Liver transplantation offers the opportunity to treat both HCC and the underlying liver disease. However, recurrence after transplantation remains one of the greatest challenges and is largely driven by tumour biology rather than tumour size alone.
Historically, transplant eligibility has relied on criteria such as the Milan criteria, which define acceptable tumour burden. While these criteria have produced excellent outcomes, they may exclude patients who could benefit from transplantation and have limited ability to predict recurrence risk.
This review explores newer approaches incorporating tumour biology, biomarkers and expanded selection criteria to improve risk assessment.
The authors synthesised evidence from contemporary observational studies, systematic reviews, meta-analyses and consensus guidelines to provide an up-to-date overview of HCC recurrence following liver transplantation
Tumour Biology is Emerging as a Key Predictor
Traditional criteria based on tumour size and number remain important but have limitations. Features associated with higher recurrence risk include:
- Large tumour burden
- Poor differentiation
- Microvascular invasion
- Elevated tumour markers
Expanded criteria, including:
- Up-to-7 criteria
- Kyoto criteria
- Asan criteria
- HALT-HCC score
attempt to incorporate biological features alongside tumour burden and may safely expand transplant access in selected patients.
Biomarkers May Improve Risk Prediction
AFP remains the most widely used biomarker, but limitations include variable expression and confounding by inflammation or liver disease. Emerging markers include:
- PIVKA-II
- Inflammatory markers such as neutrophil-to-lymphocyte ratio
- Circulating tumour DNA
- MicroRNAs
- Gene expression signatures
These approaches may enable earlier identification of aggressive disease and more personalised surveillance.
Downstaging Can Expand Transplant Eligibility
Locoregional therapies can reduce tumour burden and allow selected patients outside standard criteria to undergo transplantation. Evidence suggests that patients successfully downstaged to within acceptable criteria can achieve outcomes comparable to standard transplant candidates, although careful selection remains essential.
Post-Transplant Management Remains Complex
Immunosuppression requires balancing graft protection with cancer control. Higher early exposure to calcineurin inhibitors has been associated with increased recurrence risk, while mTOR inhibitors may have potential anti-tumour benefits, although evidence remains mixed.
Recurrence Surveillance and Treatment
Most recurrences occur within the first two years after transplantation and are frequently extrahepatic, particularly involving the lungs. Risk-adapted surveillance strategies incorporating:
- CT/MRI imaging
- AFP monitoring
- RETREAT score assessment
may improve early detection. Treatment options depend on recurrence pattern and include:
- Surgical resection
- Thermal ablation
- TACE
- Radioembolisation
- Systemic therapies
Immune checkpoint inhibitors remain challenging due to the risk of graft rejection.
Click image to enlarge
×
Interpretation
The future of HCC transplantation is moving beyond rigid size-based criteria towards personalised risk assessment. By integrating tumour biology, biomarkers and patient-specific factors, clinicians may better balance transplant access with recurrence risk and optimise outcomes in this increasingly complex field.
Why is this Relevant for South African Practitioners
In South Africa, where donor organs are scarce and transplant resources constrained, accurate recurrence prediction is critical to maximising benefit from each available organ. This review highlights that moving beyond size-based selection criteria towards biology-driven, personalised risk assessment may allow clinicians to better identify which patients are most likely to benefit from transplantation, supporting more equitable and effective use of limited donor organs in local transplant practice.

