This document is based on original research published in JAMA, 2025. The study details are as follows: Hsu CY, Gao Y, Freedman BI, Lunn MR, Muiru AN, Schnitzler MA, Divers J, Mannon RB, Palmer ND, Karger AB, Lentine KL, Park M; Long-Term Kidney Transplantation Outcomes Network (APOLLO) Consortium. Apolipoprotein L1 Gene Genotype and Kidney Outcomes After Living Kidney Donation. JAMA Intern Med. 2026 Jun 22:e260996. doi: 10.1001/jamainternmed.2026.0996. Epub ahead of print. PMID: 42329639; PMCID: PMC13288191.
×
Copyright
This summary was prepared by The Medical Education Network based on published peer-reviewed research. The content on this page is intended as a summary and in no way should replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. Please see the Disclaimer at the end of this page for more information.
×
Publication Information
Published: 2025
Author: The Medical Education Network
Platform: www.meded.co.za
This summary was prepared by The Medical Education Network based on published peer-reviewed research. The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.
Key Takeaway
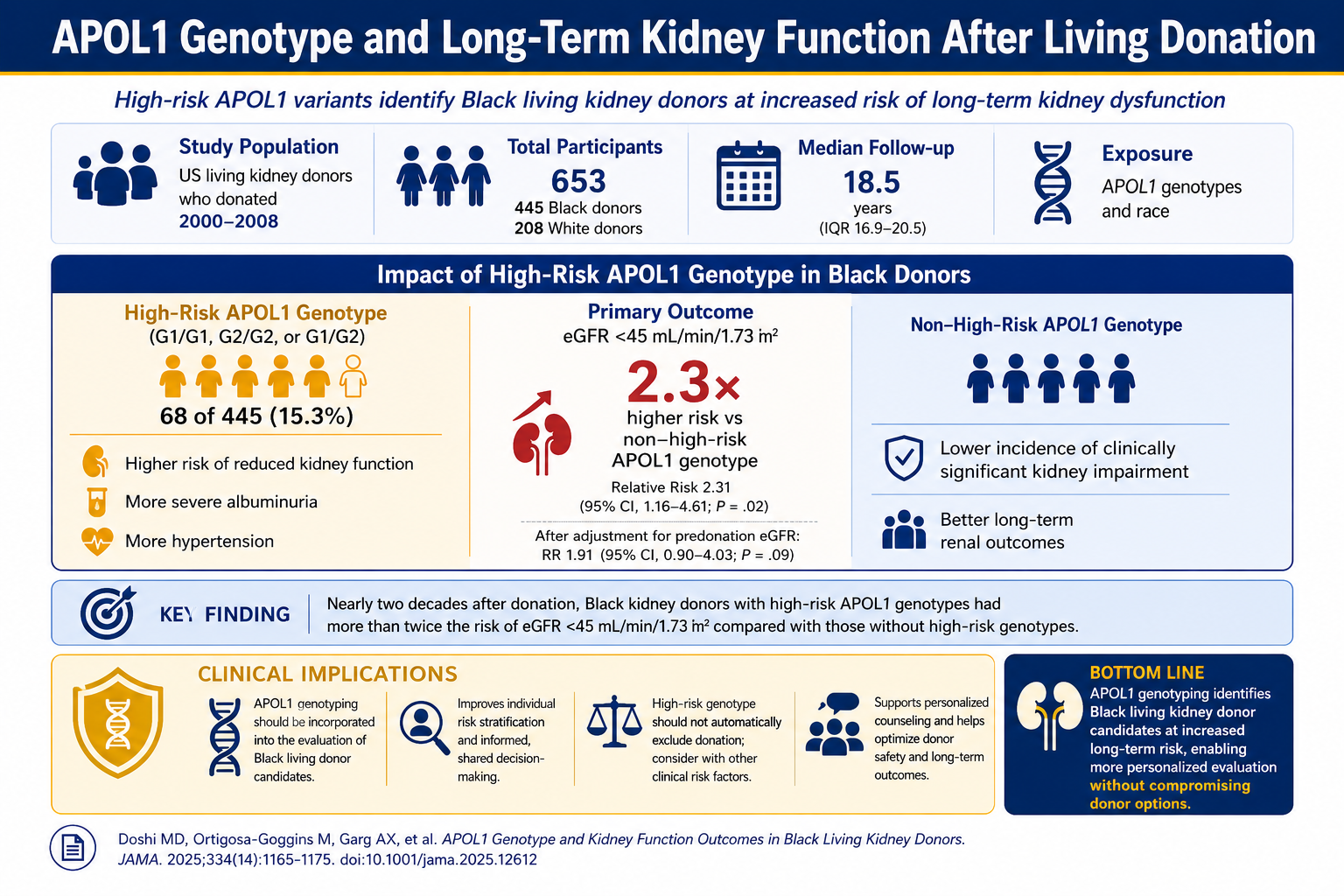
In this national US cohort study following Black living kidney donors for nearly two decades, those carrying APOL1 high-risk genotypes had more than twice the risk of significant kidney function decline compared with Black donors without these variants. The findings support routine APOL1 genotyping for all Black living donor candidates as part of comprehensive risk stratification, while stopping short of recommending it as an automatic barrier to donation.
Quick View — Key Data at a Glance
StudyRetrospective cohort (LETO ancillary study) · Scientific Registry of Transplant Recipients (USA) · 445 Black donors, 208 White donors
Study PeriodDonation 2000–2008; home visits 2020–2024
Median Follow-up18.5 years post-donation
APOL1 High-Risk Prevalence15.3% of Black donors (68/445)
Primary OutcomeeGFR <45 mL/min/1.73 m²: 14.7% (high-risk) vs 6.4% (non-high-risk)
Unadjusted RR2.31 (95% CI, 1.16–4.61; P = .02)
Severe AlbuminuriaRR 3.84 (95% CI, 1.11–13.22) for UACR ≥300 mg/g
Age EffectRR 4.19 in donors aged >38 at donation vs RR 0.82 in younger donors
Key MessageAPOL1 high-risk genotype is a significant risk factor for reduced kidney function after living donation in Black donors. Universal genotyping is warranted for risk stratification within a shared decision-making framework — not as a gatekeeping tool, but as essential information for informed consent.
Rigorous, evidence-based policies for living donor candidate selection require accurate data on long-term postdonation outcomes. Such data have historically been limited by short follow-up periods and underrepresentation of racial and ethnic minority groups.
Black donors carry a disproportionately higher risk of post-donation chronic kidney disease (CKD) and end-stage kidney disease (ESKD) compared with White donors, at two- to threefold higher rates in administrative data analyses. The apolipoprotein L1 gene (APOL1) — which harbours variants (G1 and G2) conferring increased CKD risk in individuals with recent African ancestry — is a plausible biological explanation for this disparity. However, routine APOL1 genotyping of Black donor candidates remains controversial and is not yet standard practice at many transplant centres.
Study Objective: To determine whether APOL1 high-risk genotypes (G1/G1, G2/G2, or G1/G2) are associated with worse kidney function outcomes in a US-national sample of Black living kidney donors assessed approximately 18 years post-donation.
Study Methodology
The Living Donor Extended Time Outcomes (LETO) study is a retrospective cohort ancillary to the NIDDK-funded APOLLO trial.
Participants: 445 Black donors (from 136 transplant centres) and 208 White donors (from 76 centres).
APOL1 genotyping was performed at a CLIA-certified laboratory for G1 (rs73885319; rs60910145) and G2 (rs71785313) variants using TaqMan assays. Participants with two kidney risk alleles (G1/G1, G2/G2, or G1/G2) were classified as high-risk.
Primary outcome: eGFR <45 mL/min/1.73 m² at the time of the home visit, using the 2021 CKD-EPI creatinine equation Secondary and tertiary outcomes: eGFR <60 mL/min/1.73 m²; urinary albumin-creatinine ratio (UACR) ≥30 or ≥300 mg/g; hypertension
Modified Poisson regression with robust variance was used to calculate relative risks. An adjustment was made for pre-donation eGFR where differential distribution was identified between APOL1 groups.
Study Findings
Among 445 Black living kidney donors assessed at a median of 18.5 years post-donation, 68 (15.3%) carried APOL1 high-risk genotypes. At the time of the home visit, Black donors with high-risk genotypes had significantly worse kidney outcomes across multiple measures, as shown in the interactive chart below.
Interactive Data · LETO Study · 445 Black Living Kidney Donors
APOL1 High-Risk Genotypes and Kidney Outcomes After Living Donation
Retrospective cohort · Median 18.5 years post-donation · Scroll over bars to view figures
APOL1 high-risk (G1/G1, G2/G2, G1/G2)
Without high-risk genotype
Reading this chart: Each pair of bars compares the proportion of Black living kidney donors who reached each adverse outcome threshold — those with APOL1 high-risk genotypes (navy) versus those without (blue). Higher bars indicate a greater proportion of donors in that group reaching the outcome.
2.31×
Unadjusted relative risk for eGFR <45 mL/min/1.73 m² (95% CI: 1.16–4.61)
3.84×
RR for severe albuminuria (UACR ≥300 mg/g) — significant after adjustment
For the primary outcome of eGFR <45 mL/min/1.73 m², 14.7% of high-risk donors versus 6.4% of donors without high-risk genotypes met this threshold (unadjusted RR 2.31; 95% CI, 1.16–4.61; P = .02). After adjusting for pre-donation eGFR — which was already lower at baseline in the high-risk group — the relative risk attenuated to 1.91 (95% CI, 0.90–4.03; P = .09), with the confidence interval crossing the null.
For eGFR <60 mL/min/1.73 m², high-risk donors had a 50% higher risk (RR 1.50; 95% CI, 1.18–1.90), which remained statistically significant after adjustment (adjusted RR 1.34; 95% CI, 1.08–1.67). Severe proteinuria (UACR ≥300 mg/g) was nearly four times more common in the high-risk group (RR 3.84; 95% CI, 1.11–13.22).
In age-stratified analysis, the association between APOL1 high-risk genotype and eGFR <45 mL/min/1.73 m² was markedly stronger among donors older than the median age of 38 years at donation (RR 4.19; 95% CI, 1.82–9.63) compared with younger donors (RR 0.82; 95% CI, 0.19–3.48).
Three donors (all Black) progressed to ESKD over the follow-up period; one was in the APOL1 high-risk group. Carriers of a single APOL1 risk variant (G1/G0 or G2/G0) did not have higher rates of adverse outcomes than those with no risk variants.
Clinical Takeout
These findings provide the most robust long-term evidence to date that APOL1 high-risk genotypes confer meaningful additional kidney risk after living donation in Black individuals. The unadjusted doubling of risk for eGFR <45 mL/min/1.73 m² — in a cohort assessed nearly two decades post-donation — adds to a growing body of evidence that donor selection frameworks must account for genetic risk beyond race alone.
The attenuation of the primary outcome after adjusting for pre-donation eGFR is not necessarily reassuring: the investigators argue that lower pre-donation eGFR in the high-risk group is itself likely a consequence of APOL1 genotype, meaning adjustment may obscure rather than clarify the true causal effect.
The findings support universal APOL1 genotyping for all living donor candidates with recent African genetic ancestry. Critically, however, the authors emphasise that a high-risk result should not be an automatic bar to donation. For the approximately 85% of Black candidates without high-risk genotypes, genotyping may actually provide reassurance and facilitate donation. For those with high-risk genotypes, the information enables individualised risk communication, shared decision-making, and appropriate long-term surveillance planning.
Key insight: APOL1 genotyping should become standard in the evaluation of Black living kidney donor candidates, not as a gatekeeping tool, but as essential information for accurate risk stratification and informed consent.
What This Means for South African Practitioners
South Africa’s transplant landscape makes these findings particularly relevant. Kidneys available for transplantation are scarce, and in a healthcare environment where access to long-term dialysis in the public sector remains constrained, the long-term health of living donors demands careful, equitable attention.
Local data on APOL1 variant prevalence in South African populations is beginning to emerge. A 2023 master’s dissertation from the University of the Free State (Notani MD, UFS2) examined APOL1 G1 and G2 variant frequencies in 220 participants of African descent in Bloemfontein, across four groups stratified by HIV status and the presence of kidney disease indicators. The study found that all tested APOL1 risk variants were present in this South African population and notably that the G2 variant was more prevalent than G1, a pattern that differs from the 1000 Genomes Africa reference frequencies. The G2/G2 frequency in this cohort (0.0455) was higher than the 1000 Genomes Africa benchmark (0.017), while G1/G1 frequency (0.0045) was markedly lower than the reference (0.080).
Taken together: The LETO study establishes that APOL1 high-risk genotypes meaningfully increase long-term kidney risk after living donation in Black individuals, while the UFS data confirm that all relevant variants are present and detectable in South African populations of African ancestry. The different G1/G2 prevalence pattern observed locally compared with US and global reference data also suggests that South African-specific prevalence data — rather than extrapolation from North American cohorts — will ultimately be needed to guide local donor risk frameworks.
The key message for local clinicians is that genotyping is about improving informed consent and shared decision-making, not excluding donors, and that a high-risk result should trigger enhanced post-donation monitoring rather than automatic disqualification. The age-stratified findings from LETO are particularly actionable: the markedly higher risk in donors older than 38 suggests that age and genotype together should inform the risk discussion in a way that neither factor alone can achieve.
As transplant programmes continue to evolve in South Africa, integrating genetic risk assessment into donor evaluation — where feasible and accessible — represents a meaningful step toward more equitable, evidence-based donation practice.
Notani MD. Prevalence of APOL1 risk variants in HIV-positive compared to HIV-negative individuals with evidence of kidney disease. MSc dissertation (Genetics), University of the Free State, Bloemfontein, 2023. Available at: https://scholar.ufs.ac.za/items/e9f0f4c1-1df1-400e-82b9-683dc5d140b9 [Accessed June 2025]
Disclaimer
This summary was prepared by The Medical Education Network based on published peer-reviewed research. The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.