This document is based on original research published in the SAMJ, 31 May 2022. The study details are as follows: Jauquier N, English N, Davidson A, Cox SG. Solid malignancies during the first year of life: A 20-year review at Red Cross War Memorial Children's Hospital, Cape Town, South Africa. S Afr Med J. 2022 May 31;112(6):418-425. PMID: 36217871.
×
Copyright
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content on this page is intended as a summary and in no way should replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. Please see the Disclaimer at the end of this page for more information.
×
Publication Information
Published: 24 February 2026
Author: The Medical Education Network
Catalogue Number: MPCS0016
Platform: www.meded.co.za
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.
×
Click image or press Esc to close
Key Takeaway
A South African tertiary centre demonstrated that protocol-driven multidisciplinary care for infantile solid malignancies achieves survival outcomes comparable to high-income countries, validating that resource-appropriate application of international treatment guidelines delivers world-class paediatric oncology care in middle-income settings.
Quick View — Key Data at a Glance
Study 20-year retrospective series · RCWMCH · 122 infants <1 year
Study Period January 1997 – December 2016
Most Common Tumour Renal 31.2% — ahead of neuroblastoma (24.6%)
Most Challenging Non-rhabdomyosarcoma soft-tissue sarcomas 54.2%
Key Message Protocol-driven multidisciplinary care in a middle-income setting achieves survival outcomes equivalent to high-income countries — outcomes are determined by the right team and the right protocols, not by geography.
Paediatric malignancies are rare, representing approximately 1% of all new tumour diagnoses annually. Within this already small cohort, neonatal and infantile tumours form an even more distinct subset — accounting for 2% and 10% of paediatric cancers respectively — and they behave in ways that set them fundamentally apart from tumours in older children or adults.1
Their pathogenesis, biological behaviour, and response to treatment all differ in clinically important ways, and this has direct implications for how these patients must be managed.
What makes infantile solid tumours particularly challenging is the combination of insidious onset and physiological vulnerability. These tumours can be present for some time before a diagnosis is even considered, and when treatment is finally initiated, the infant’s developing organ systems and limited physiological reserve demand careful dosage modification and close monitoring for developmental sequelae.
These are not simply smaller versions of adult oncology cases — they require age-specific protocols, a genuinely multidisciplinary team, and a degree of institutional experience that cannot be improvised at the bedside.
Study Objective: Conducted at Red Cross War Memorial Children’s Hospital (RCWMCH), this descriptive analysis evaluated solid non-central nervous system malignancies in children diagnosed before their first birthday, characterising tumour distribution, treatment modalities, surgical complications, and clinical outcomes within a middle-income country healthcare setting.
Study Methodology
The analysis drew on the RCWMCH oncology database and reviewed all patients diagnosed under the age of one year between January 1997 and December 2016. Of 243 cases initially extracted, 198 were confirmed solid tumours.
After excluding benign lesions and tumours of the eye, bone, and central nervous system — which fall outside the scope of this analysis — 122 patients were included.
Tumours were classified using the International Classification of Childhood Cancer, 3rd edition (ICCC-3), covering renal, neuroblastic, soft-tissue, hepatic, and germ cell malignancies. Survival outcomes were analysed using Kaplan-Meier methodology, with a mean follow-up of 46 months across the cohort.
Primary outcome: Five-year overall survival by tumour type Secondary outcomes: Tumour distribution, treatment modalities, surgical complication rates, and overall cohort mortality
Study Findings
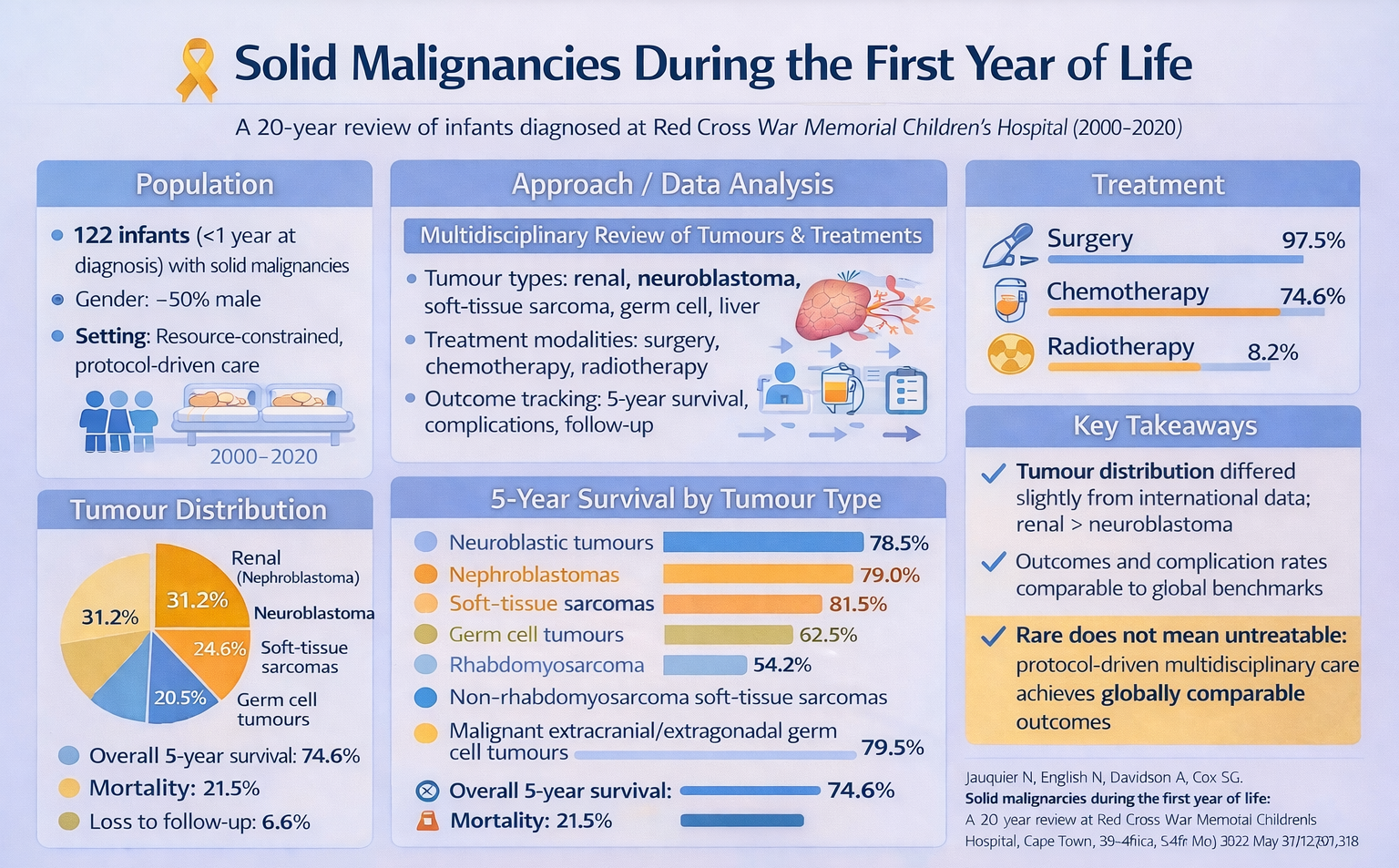
The cohort had a median age of 5.5 months and a near equal male:female ratio (1.03:1 respectively). Renal tumours were the most common presentation, comprising 38 cases (31.2%), followed by neuroblastomas at 30 cases (24.6%), soft-tissue sarcomas at 25 (20.5%), germ cell and gonadal tumours at 17 (13.9%), and hepatoblastomas at 12 (9.8%).
Click to enlarge — Quick Summary graphic
Treatment was appropriately intensive given the nature of these diagnoses. Surgery was performed in 97.5% of cases — reflecting both the primary role of resection in solid tumour management and the centre’s capacity to offer it across this full age range. Chemotherapy was administered in 74.6% of cases, while radiotherapy, used selectively given the known risks of developmental toxicity in this age group, was applied in only 8.2%.
Survival outcomes were notably strong across most tumour types. Nephroblastoma achieved a five-year overall survival of 79.0%, neuroblastic tumours 78.5%, hepatoblastomas 81.5%, and malignant extracranial and extragonadal germ cell tumours 79.5%.
Soft-tissue sarcomas showed more modest results, with rhabdomyosarcoma reaching 62.5% and non-rhabdomyosarcoma soft-tissue sarcomas 54.2% — consistent with the known difficulty of achieving local control in these entities at any age, compounded further by the treatment constraints that apply in the first year of life.
Across the entire cohort, five-year overall survival was 74.6%, with a mortality rate of 21.5%, loss to follow-up of 6.6%, and a surgical complication rate of 10.9%.
Clinical Takeout
Two findings from the study are worth reflecting on:
The first is the tumour distribution itself: renal tumours predominated over neuroblastomas — the reverse of what is typically reported in international literature. Whether this reflects a genuine regional epidemiological pattern, a referral bias particular to RCWMCH’s catchment, or a data artefact from the retrospective design is not fully resolved by this study, but it is a consistent enough finding to warrant attention in future South African series.
The second, and arguably more important, finding is what the survival data says about what is achievable within a resource-constrained middle-income setting. A 10.9% surgical complication rate and a 74.6% five-year overall survival are both figures that sit comfortably within published international benchmarks — not as approximations, but as genuine equivalents. This is not a coincidence. It is the direct result of applying structured, protocol-driven management through a dedicated multidisciplinary team. For clinicians working in South African public sector settings, that is perhaps the most actionable message this study offers: outcomes are not determined by geography or GDP, but by whether the right team, with the right protocols, sees the patient early enough to make a difference.
Key insight: Protocol-driven multidisciplinary care in a middle-income setting achieves survival outcomes equivalent to high-income countries — outcomes are determined by the right team and the right protocols, not by geography.
What This Means for South African Practitioners
This analysis demonstrates that resource-appropriate application of international treatment protocols by dedicated multidisciplinary teams can achieve outcomes comparable to high-income countries. For South African clinicians encountering these rare infantile presentations, early referral to specialised centres remains the single most consequential intervention available.
The rarity of these tumours — solid non-CNS malignancies presenting before the first birthday — must be understood within South Africa’s broader paediatric oncology landscape, which itself carries significant structural challenges. Paediatric cancers overall account for approximately 13.5% of all cancers in children in South Africa, with kidney tumours (nephroblastoma/Wilms tumour) consistently ranking among the top five malignancies in both boys and girls according to National Cancer Registry and SACCSG data.4
Yet despite this relative prevalence at the population level, the infantile solid tumour cohort examined at RCWMCH represents a distinctly rare subset — one that demands highly specialised surgical and oncological expertise that is not uniformly distributed across the country.
The South African healthcare system is deeply bifurcated. Private medical aid coverage has historically remained between 15% and 18% of the total population, and in 2015, only 13.5% of children with cancer were managed in private paediatric oncology units.3 The majority of paediatric oncology care is delivered in the public sector, where units grew from eight in 2002 to thirteen by 2017 — a welcome expansion, but one that still leaves wide geographic gaps, particularly for patients in rural provinces and neighbouring countries such as Lesotho.3 This inequity in service distribution directly affects whether families can access the kind of specialised, protocol-driven care that the RCWMCH series demonstrates is possible.
Diagnostic delay compounds these structural challenges. A recent 21-year retrospective analysis of nephroblastoma at Universitas Academic Hospital (Bloemfontein) found a median one-month delay between symptom onset and diagnosis, driven by delayed care-seeking, limited primary healthcare awareness, and socioeconomic barriers.2 The same study observed a stage IV disease rate of 29.5% — considerably higher than comparable South African series — with five-year survival of 59.4%, markedly lower than the 79% nephroblastoma survival reported in the RCWMCH infantile cohort.2 This disparity underscores what centralised, protocol-adherent specialist care can achieve, but it also highlights how much is lost when that care is accessed late or not at all.
For the rare infantile tumours described in this study, these delays carry even greater consequences. The insidious onset of neonatal and infantile malignancies, combined with low primary-care awareness of their existence, means that most presentations will first be encountered by generalist or community-level clinicians who may not immediately consider malignancy in a child under twelve months. The 10.9% surgical complication rate reported in this cohort is manageable within a specialist centre; in a non-specialist setting, it would likely be considerably higher.
Brain tumours represent a useful parallel: while they constitute approximately 25% of childhood cancers in developed countries, South African SACCSG data records only 13.4% — a discrepancy attributed largely to under-diagnosis, particularly in smaller and rural hospitals.4 A similar blind spot may exist for rare infantile solid tumours, where true incidence is likely underestimated due to gaps in registry coverage.3 The South African Children’s Tumour Registry (SACTR) and the National Cancer Registry (SA-NCR) remain the most reliable data sources, but the absence of comprehensive, population-based data limits our ability to determine whether the RCWMCH distribution — where renal tumours predominated over neuroblastomas — is a regional pattern, a referral bias, or a true epidemiological signal.3
Importantly for our resource-restrained context, the RCWMCH data reinforces that middle-income healthcare systems can deliver world-class paediatric oncology outcomes when structured protocols guide practice and when cases are concentrated in experienced centres.2 The policy imperative that follows is clear: investment in regional referral pathways, primary care training in early cancer recognition, and strengthening of national tumour registries are not aspirational goals — they are the levers most likely to close the gap between what is achievable, as demonstrated by this study, and what is currently being achieved across the country.3
1. Zhi T, Zhang WL, Zhang Y, Wang YZ, Huang DS. Prevalence, clinical features and prognosis of malignant solid tumors in infants: a 14-year study. Bosnian Journal of Basic Medical Sciences. 2021;21(5):598–606. https://doi.org/10.17305/bjbms.2020.5121
2. Brits E, Gerber E, Iroka I, et al. Paediatric nephroblastoma at a South African tertiary hospital: A 21-year retrospective analysis. S Afr Med J. 2024;114(12):e2223. https://doi.org/10.7196/SAMJ.2024.v114i12.2223
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.