This document is based on original research published in JAMA Network Open, 4 March 2026. The study details are as follows: Yu ME, Husain SA, Tucker EG, et al. Expedited Transplant Allocation Using a Paired Kidney Cohort. JAMA Netw Open. 2026;9(3):e260257. doi:10.1001/jamanetworkopen.2026.0257
×
Copyright
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content on this page is intended as a summary and in no way should replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. Please see the Disclaimer at the end of this page for more information.
×
Publication Information
Published: 4 March 2026
Author: The Medical Education Network
Catalogue Number: MEDTR001
Platform: www.meded.co.za
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content on this page is intended as a summary only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.
Key Takeaway
In this US-based study, expedited (out-of-sequence) kidney allocation increased 17-fold between 2020 and 2024, with organs being diverted from the standard queue far earlier in the match process. Yet patient and graft survival remain comparable to standard allocation, supporting the clinical safety of this strategy for improving organ utilisation.
Quick View — Key Data at a Glance
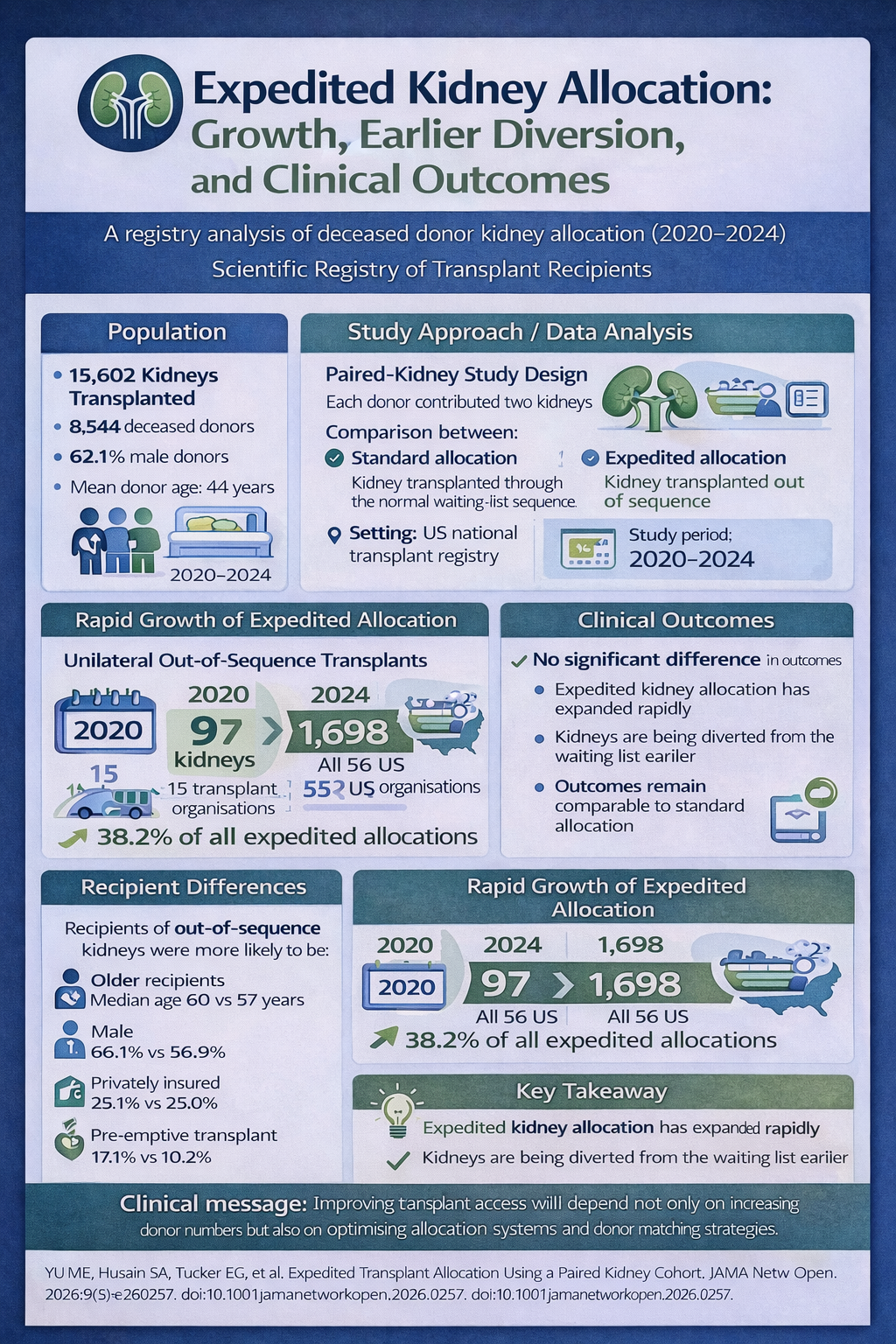
Study National registry cohort analysis · Scientific Registry of Transplant Recipients (USA) · 15 602 kidneys from 8 544 deceased donors
Study Period 2020 – 2024
Rapid Growth Unilateral out of sequence (OOS) transplants rose from 97 cases (15 OPOs) in 2020 to 1 698 cases (all 56 US OPOs) in 2024 — a 17-fold increase
Earlier Diversion Median waiting-list sequence position at first OOS diversion fell from 393 (2020) to 28 (2024)
Patient Survival HR 0.84 (95% CI 0.70–1.02) — no significant difference vs standard allocation
Graft Survival HR 0.87 (95% CI 0.70–1.08) — no significant difference vs standard allocation
Key Message Expedited kidney allocation is being used more frequently and earlier in the match process, but appears clinically safe, with survival outcomes comparable to standard allocation pathways. Recipient disparities in insurance status and pre-emptive transplant access warrant ongoing monitoring for equity.
Kidney transplantation is the preferred treatment for patients with end-stage kidney disease, offering superior survival and quality of life compared with long-term dialysis. However, demand for donor kidneys continues to far exceed supply, resulting in prolonged waiting times for transplantation in many healthcare systems.
To improve utilisation of available organs and reduce the likelihood of potentially viable kidneys being discarded, transplant programmes have increasingly adopted expedited or out-of-sequence allocation. In this approach, kidneys may be offered outside the traditional waiting-list sequence when concerns arise that the organ may otherwise go unused. While this strategy may accelerate organ placement, it has also prompted questions regarding transparency, equity of access, and whether allocation outside the standard match-run process influences transplant outcomes.
Study Objective: To examine the use and clinical outcomes of expedited (out-of-sequence) allocation of deceased donor kidneys, using a paired-kidney design that compared kidneys from the same donor — one transplanted through the standard sequence, the other out of sequence — to control for donor-related factors and more clearly assess whether the allocation pathway itself influences outcomes.
Study Methodology
This retrospective cohort study analysed data from the Scientific Registry of Transplant Recipients (SRTR) in the United States, covering deceased donor kidney transplants performed between 2020 and 2024. The analysis included 15 602 kidneys recovered from 8 544 deceased donors, with approximately 62% of donors being male and a mean donor age of 44 years.
Kidneys were categorised according to allocation pathway:
Both kidneys transplanted out of sequence
One kidney transplanted in sequence and the other out of sequence (unilateral OOS — the primary comparison group)
A single kidney transplanted out of sequence
The paired-kidney design was key to the study’s strength: by comparing kidneys from the same donor, the investigators controlled for donor-related factors that might otherwise confound outcome comparisons between allocation pathways.
Primary outcomes: Patient survival and graft survival following transplantation Secondary outcomes: Trends in OOS allocation volume, sequence position at diversion, recipient characteristics, and refusal code patterns over time
Study Findings
In a national registry analysis of 15 602 kidneys from 8 544 deceased donors, expedited kidney allocation increased dramatically over the study period, yet patient and graft survival remained comparable between kidneys transplanted within and outside the standard allocation sequence.
Of the 8 544 donors included, just over half (50.5%) had one kidney transplanted out of sequence. Unilateral out-of-sequence allocation — where one kidney from a donor was transplanted in sequence and the other was not — accounted for 38.2% of all OOS transplants during the study period. The growth was striking, as shown in the interactive chart below. (Scroll over items to view information.)
Transplant Data · USA · 2020–2024
Expedited Kidney Allocation: Growth vs Earlier Diversion
Unilateral OOS transplants surged 17-fold while kidneys were diverted from the standard queue far earlier in the match process.
Unilateral OOS Transplants
Left axis — number of kidneys
Median Sequence Position at First OOS Diversion
Right axis — waiting list position
17×
Increase in unilateral OOS transplants between 2020 and 2024
393 → 28
Median sequence position at OOS diversion, 2020 vs 2024
The point in the match run at which kidneys were diverted from the standard sequence also changed markedly. In 2020, kidneys ultimately placed out of sequence were first refused at a median position of approximately 393 candidates on the waiting list. By 2024, this had fallen to around the 28th position — indicating that organs were increasingly being allocated outside the standard sequence much earlier in the process.
Over the same period, donor-related reasons for refusal declined by approximately 10–15%, suggesting that decisions to allocate kidneys through expedited pathways may increasingly be driven by logistical considerations rather than donor quality alone.
Recipients of out-of-sequence kidneys differed in several respects from those receiving kidneys through the standard match run. They tended to be slightly older (median age 60 vs 57 years), were more frequently male, and more likely to be White or Asian. They were also more likely to have private health insurance (29.1% vs 23.0%) and to undergo pre-emptive transplantation prior to dialysis (17.1% vs 10.2%), suggesting that socioeconomic and healthcare access factors may influence which patients ultimately receive these organs.
Despite these differences in allocation patterns and recipient characteristics, clinical outcomes remained comparable. In adjusted analyses, unilateral out-of-sequence transplantation was not associated with a statistically significant difference in patient survival (HR 0.84; 95% CI 0.70–1.02) or graft survival (HR 0.87; 95% CI 0.70–1.08) compared with kidneys transplanted within the standard allocation sequence.
Click to enlarge — Study Summary Infographic
×
Click outside the image or press Esc to close
Clinical Takeout
Taken together, these findings suggest that expedited kidney allocation can be used without compromising transplant outcomes. In this paired-kidney analysis, both patient and graft survival were similar regardless of whether kidneys were transplanted through the standard match run or through expedited pathways. This supports the clinical safety of transplanting organs allocated outside the traditional sequence, particularly when doing so may help prevent organ discard.
However, the study also raises important questions regarding how and when expedited allocation is used. Because kidneys from the same donor were compared, differences in donor quality are unlikely to explain why one kidney was transplanted within the standard sequence while the other was not. The rapid expansion of unilateral out-of-sequence allocation — and the dramatic shift toward earlier diversion in the match run — therefore suggests that logistical or institutional factors may increasingly influence allocation decisions.
The findings also highlight potential concerns regarding equity in access to transplantation. Recipients of out-of-sequence kidneys were more likely to have indicators associated with greater healthcare access, including private insurance and pre-emptive transplantation. While expedited allocation may improve overall organ utilisation, these observations underscore the importance of transparent governance and clearly defined allocation criteria to ensure that transplant systems remain equitable.
Key insight: Expedited kidney allocation is clinically safe — outcomes are comparable to standard pathways — but the growing use of earlier diversion and the recipient demographic disparities observed warrant transparent allocation governance to protect equitable access.
What This Means for South African Practitioners
These considerations are particularly relevant in the South African context, where transplantation takes place within a resource-constrained healthcare environment characterised by limited organ availability and restricted access to long-term dialysis. Waiting times for deceased donor kidneys may extend for many years, and access to chronic dialysis in the public sector is often constrained by capacity limitations.
In this setting, each successful kidney transplant has broader implications for the healthcare system. Beyond improving survival and quality of life for the recipient, transplantation may also free a dialysis slot for another patient who might otherwise be unable to access life-sustaining treatment.
Innovations in donor matching and allocation therefore have considerable potential to expand transplant opportunities in South Africa. One promising approach is kidney paired donation, in which incompatible donor–recipient pairs are matched with other pairs to enable compatible exchanges. Through this strategy, patients who would otherwise be unable to receive a transplant because of immunological incompatibility may undergo transplantation without requiring complex desensitisation protocols.
Early paired-donation initiatives in South Africa have demonstrated that such exchanges are feasible and can facilitate transplantation for patients who previously had limited treatment options. As transplant programmes continue to evolve, expanding collaborative matching systems and strengthening allocation frameworks may represent important steps toward improving access to transplantation.
Ultimately, the findings of this study reinforce a broader principle in transplant medicine: improving access to transplantation will depend not only on increasing donor numbers but also on optimising allocation systems and matching strategies. For healthcare systems with constrained resources, such as South Africa’s, transparent allocation policies and innovative approaches such as kidney exchange programmes may play an important role in ensuring that the limited supply of donor organs benefits as many patients as possible.
This summary was extracted from an open-access article distributed under the terms of the CC-BY license, which permits unrestricted use, distribution, and reproduction in any medium. The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.