Clinical motor and sensory examination moderately predicts spinal injury, but imaging (CT and MRI) remains essential to accurately identify injury level and detect subtle or soft-tissue injuries.
Quick Facts
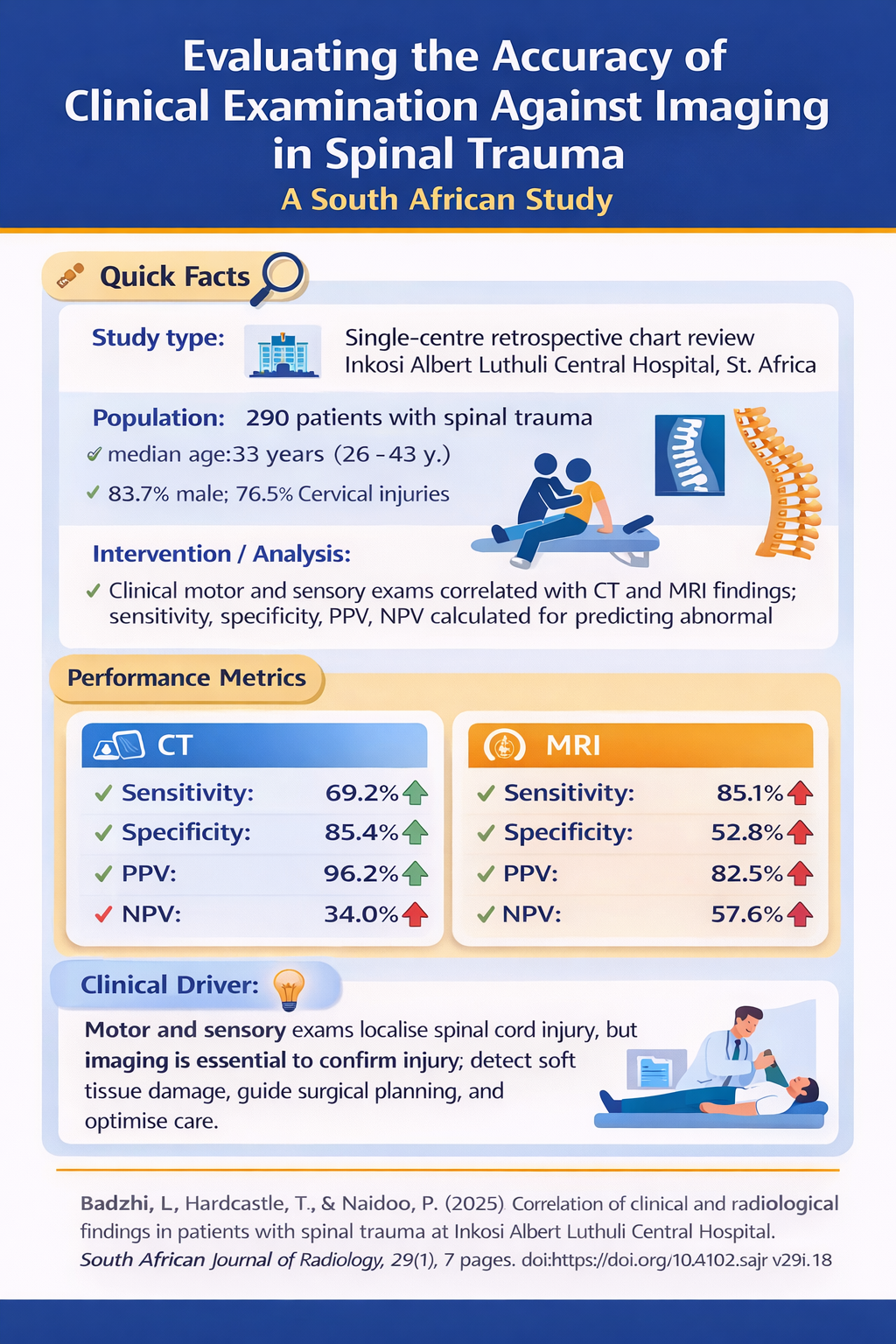
Study type: Single-centre retrospective chart review (Inkosi Albert Luthuli Central Hospital, 6 years) Population: 290 patients with spinal trauma (median age 33 years; 83.7% male; 76.5% cervical injuries) Interventions / Analysis: Clinical motor and sensory examination correlated with CT and MRI findings; sensitivity, specificity, PPV, NPV calculated for predicting abnormal imaging Key result: Clinical findings reasonably predict abnormal imaging but cannot reliably exclude injury; CT best for bony injuries, MRI best for soft tissue and spinal cord evaluation Performance metrics:
Spinal trauma is increasingly common in South Africa, particularly among young males.
In this recent study of 290 patients with spinal cord injuries (SCI) at Inkosi Albert Luthuli Central Hospital, 83.7% were male with a median age of 33 years. Cervical spine injuries dominated (76.5%), with thoracic injuries accounting for 13.8% and lumbo-sacral or multilevel injuries comprising approximately 10% of all injuries seen. Vehicle-related mechanisms (motor vehicle collisions and pedestrian vehicle crashes) caused 61.8% of injuries. Polytrauma was the norm rather than the exception: over 70% had concurrent brain injuries, 37.5% chest injuries, 28.6% abdominal injuries, and 37.2% limb injuries.
Diagnosis of spinal cord injury (SCI) in resource-limited settings remains challenging for EM practitioners.
Assessment of spinal trauma traditionally relies on a comprehensive neurological examination using the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) and the ASIA Impairment Scale. However, questions remain regarding the concordance between clinical findings and radiological results, and whether advanced imaging is always required—particularly in settings where access to such resources is constrained.
Study Objective
In response to these challenges, the researchers of this study sought to evaluate whether clinical motor and sensory findings correlate with imaging results, to determine whether imaging is always necessary, and to compare the predictive accuracy of clinical versus radiological assessment in patients with spinal trauma.
Study Methodology
The study was a retrospective chart review of 290 patients with spinal injuries admitted over six years (2018–2024) who received CT and/or MRI. Motor and sensory examination findings were compared against radiological results.
Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated to assess the clinical examination's ability to predict abnormal imaging findings.
Study Findings
Clinical motor and sensory findings demonstrated a high positive predictive value, but there were concerning limitations in ruling out injury.
For CT imaging, clinical findings showed 69.2% sensitivity, 85.4% specificity, 96.2% PPV, but only 34.0% NPV. For MRI, sensitivity improved to 85.1%, with 52.8% specificity, 82.5% PPV, and 57.6% NPV.
Clinical findings correlated with abnormal CT results in 84.4% of cases and with MRI in 72.3%—suggesting reasonable agreement but revealing a critical gap: clinical examination frequently overestimated the injury level or position.
The low negative predictive values (34.0% for CT, 57.6% for MRI) indicate that negative clinical findings cannot reliably exclude spinal injury.
CT proved superior for detecting bony injuries, fractures, subluxations, and dislocations, while MRI was essential for identifying soft tissue pathology—including posterior and anterior ligamentous injuries, spinal cord oedema, haemorrhage, and disc ruptures.
Some patients presented with Spinal Cord Injury Without Radiographic Abnormality (SCIWORA), where neurological deficits existed despite normal CT findings, making MRI crucial for diagnosis.
Interpretation
Clinical examination alone cannot reliably exclude spinal injury and tends to overestimate injury level. The low negative predictive values mean that normal motor and sensory findings do not adequately rule out significant pathology. Imaging remains essential: CT for bony assessment and MRI for soft tissue, ligamentous, and spinal cord evaluation. Combined clinical and radiological assessment provides the most accurate foundation for management decisions, including surgical intervention (favoured within 24 hours for unstable fractures), conservative treatment, and coordinated multidisciplinary care.
Why This is Relevant for South African Practitioners
Trauma is a public health crisis in South Africa, with transport-related injuries and interpersonal violence predominating—yet many tertiary public hospitals lack dedicated trauma teams.1 While spinal cord injury surveillance data remains scanty, Gauteng Province reports the highest proportion of assault-related traumatic SCI worldwide. 2 That said, KwaZulu-Natal and the Eastern Cape have the highest numbers of people living with SCI. 3
The findings of this study emphasise the need to maintain a consistently high index of suspicion in all suspected cases of spinal cord injury. Clinical examination alone cannot safely exclude significant pathology, particularly in frontline and rural settings. Where imaging is unavailable, early referral to appropriately equipped centres is essential to prevent missed injuries and avoidable neurological deterioration.
From a public health perspective, the implications are equally important. In under-resourced settings where access to advanced imaging is uneven, limited diagnostic capacity risks widening disparities in care. Strengthening referral systems, improving access to imaging, and supporting coordinated multidisciplinary management are critical steps toward ensuring equitable spinal trauma care and advancing universal access to treatment.
Disclaimer:
The content in this summary is intended as an overview only and does not replace the original research. Members should review the original study before forming clinical opinions. The Medical Education Network cannot be held liable for inaccuracies or omissions.
Fact-checking Policy:
The Medical Education Network makes every effort to review and fact-check source material. Please use the contact us form to report issues.
×
Publication Information
Published: 2 February 2026
Author: The Medical Education Network
Platform: www.meded.co.za
Originally Published: SA Radiology Journal, 20 December 2025 The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions.
×
Original Research
Badzhi, L., Hardcastle, T., & Naidoo, P. (2025). Correlation of clinical and radiological findings in patients with spinal trauma at Inkosi Albert Luthuli Central Hospital. South African Journal of Radiology, 29(1), 7 pages. doi:https://doi.org/10.4102/sajr.v29i1.3248
×
Copyright
The content in this summary is intended as an overview only and does not replace the original research. The Medical Education Network strongly encourages all members to review the original study before forming clinical opinions or making decisions. While every effort has been made to accurately represent the study’s findings, any errors are unintentional, and the Medical Education Network cannot be held liable for any inaccuracies or omissions. If you have any queries regarding this article contact us.