
Pertussis on the rise: misunderstood, misdiagnosed and lethal
Published on MedED: 28 August 21
Type of article: Original Article
MedED Catalogue Reference: MPN002
Compiler: Linda Ravenhill
Sources: BMC Pediatrics, BMJ Open, Expert Review of Vaccines, CDC.gov
Type of article: Original Article
MedED Catalogue Reference: MPN002
Compiler: Linda Ravenhill
Sources: BMC Pediatrics, BMJ Open, Expert Review of Vaccines, CDC.gov
Pertussis was first described in1578 by French physician Guillaume De Baillou. He named the disease ‘quinte’ when describing an epidemic in Paris at that time. But it was not until 1906 that the causative organism – the highly contagious bacterium Bordetella pertussis - was isolated by Belgian immunologist Jules Bordet and Belgian bacteriologist, Octave Genou.4
Today, pertussis is one of the most common childhood diseases and sadly one of the most significant contributory causes of childhood mortality.4 It is considered a cyclical endemic disease, with outbreaks believed to occur every 3 - 6 years. It affects all ages, but the highest mortality is in infants younger than three months.3 In 2013, the Global Burden of Disease Study estimated mortality in the first year of life resulting from pertussis to be “..approximately 400 per million live births, or approximately 56,000 deaths annually."3
And yet pertussis is vaccine-preventable.
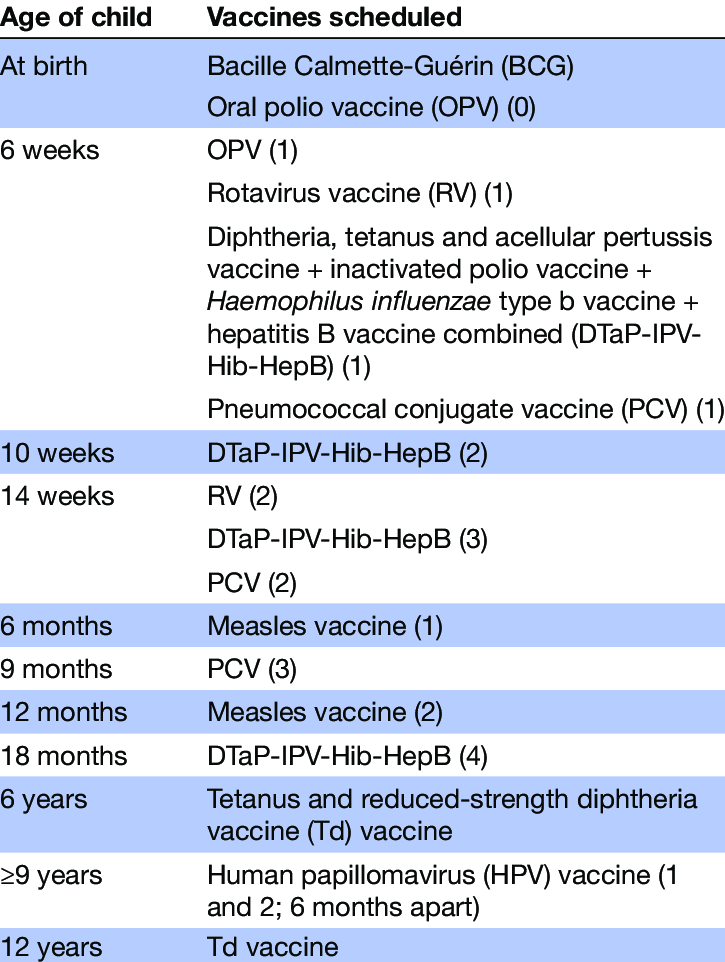
The Global Vaccine Action Plan put in place by the WHO in 2012 saw 194 signatories - of which South Africa was one - commit to a least a 90% national coverage of the Tetanus, Diphtheria and Pertussis (Tdap) vaccination in all countries, for children younger than one year, by the year 2015.6 Tdap vaccination is part of the South African Department of Health immunisation strategy, and South Africa had further set a goal of achieving at least 92% national coverage by 2017. A paper by Wiysonge et al., published in BMJ Open in 2020, however, noted that the South African Demographic and Health Survey of 2016 indicated DTP3 coverage to be only 66%. 6
Figure 1. Expanded Program on Immunisation Schedule in South Africa6
Despite all these efforts, pertussis is on the rise globally, a phenomenon referred to as “resurgence pertussis”. 5
This is not only occurring in developing countries such as South Africa but there has been a marked increase in pertussis in developing nations, regardless of effective immunization programs.
Kandeil et al. attribute this resurgence to multiple factors, including “..increased disease awareness and improved diagnosis, faster waning of immunity following vaccination with aP compared to wP vaccines, and/or genetic changes in the bacterium.”3
Many of the deaths attributable to pertussis infant mortality occur in those too young to be vaccinated and thus rely on maternal antibody transfer for initial immune response.
Wang et al. go further, attributing the high rate of disease mortality in infants to two factors: a lack of sufficient understanding of the clinical characteristics and risk factors for severe pertussis among treating physicians, who often do not recognise or focus their attention on these factors, and a lack of clarity surrounding the pathogenesis and lethality mechanisms of pertussis. 5
.
Pertussis follows three stages –catarrhal, paroxysma and finally convalescence. The full spectrum of the disease can last up to 6- 12 weeks.2
Figure 2: Clinical Course of Pertussis2
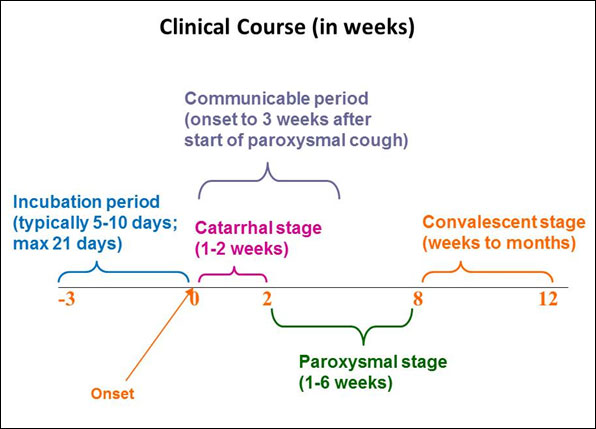
Source: Center for Disease Control and Prevention. 2019. Pertussis ( Whooping Cough). 2
The initial stages present with mild cold-like symptoms- a slight cough, low-grade fever, and catarrh - usually within 14 days from exposure. Because of this insidious onset, the disease is often misdiagnosed by practitioners, until the characteristic inspiratory “whoop”, at the end of the paroxysmal cough, which occurs in the second stage of the disease. 2
Infants, in particular, are most likely to present with a cough with or without paroxysms, cyanosis, apnea, tachypnea, difficulty in breathing and leukocytosis.1. For many, apnea may be the only sign of the disease during this second stage, and those younger than 12 months are most at risk during this period.1
Pneumonia is the most common complication of pertussis and is the leading cause of severe disease and death from pertussis. Other complications include: Pertussis encephalopathy and heart failure. 3
Practitioners are wise to consider the presence of pertussis in young neonates and children who present with these initial symptoms to commence treatment early and reduce the rate of complications. Furthermore, there is an important role to be played by all healthcare practitioners to encourage vaccination – both in mother and child, to reduce the burden of disease.
Access the original source articles here
 Analysis of clinical characteristics of severe pertussis in infants and children: a retrospective study
Analysis of clinical characteristics of severe pertussis in infants and children: a retrospective study
A systematic review of the burden of pertussis disease in infants and the effectiveness of maternal immunization against pertussis
Contextualised strategies to increase childhood and adolescent vaccination coverage in South Africa: a mixed-methods study
Analysis of clinical characteristics of severe pertussis in infants and children: a retrospective study A systematic review of the burden of pertussis disease in infants and the effectiveness of maternal immunization against pertussisContextualised strategies to increase childhood and adolescent vaccination coverage in South Africa: a mixed-methods study You may find the below-associated content of interest
Safety of Maternal Immunization Against Pertussis: A Systematic Review
Safety of Maternal Immunization Against Pertussis: A Systematic Review References:
1.Agrawal, A, S Singh, S Kolhapure, W Kandeil, R Pai, and T Singhal. 2019. “Neonatal Pertussis, an Under-Recognized Health Burden and Rationale for Maternal Immunization: A Systematic Review of South and South-East Asian Countries.” Infect Dis Ther 8 (2): 139–153. Accessed August 27, 2021. doi:10.1007/s40121-019-0245-2. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6522626/
2. Center for Disease Control and Prevention. 2019. Pertussis ( Whooping Cough). 25 October. Accessed August 25, 2021. Retrieved from https://www.cdc.gov/pertussis/clinical/features.html.
3. Kandeil, W, E M Bunge, V A Jenkins, M A Ceregido, and A Guignard. 2020. “A systematic review of the burden of pertussis disease in infants and the effectiveness of maternal immunization against pertussis.” Expert Review of Vaccines 19 (7): 621-638. Accessed Aug 28, 2021. doi:https://doi.org/10.1080/14760584.2020.Retrieved from https://www.tandfonline.com/doi/full/10.1080/14760584.2020.1791092?src=recsys
4. Moro, L P, P F Havers, S Hariri, and S Skoff. 2021. Epidemiology and Prevention of Vaccine-Preventable Diseases. Edited by Center for Communicable Diseases. Vol. 14. https://www.cdc.gov/vaccines/pubs/pinkbook/index.html. Accessed August 27, 2021. Retireved from https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/pert.pdf.
5. Wang, C, H Zhang, Y Zhang , L Xu, M Miao, H Yang, Y Liu, S He, and L Pang . 2021. “Analysis of clinical characteristics of severe pertussis in infants and children: a retrospective study.” BMC Pediatrics 21 (Article number: 65 (2021)). Accessed August 27, 2020. doi:https://doi.org/10.1186/s12887-021-02507-4. Retrieved from https://bmcpediatr.biomedcentral.com/articles/10.1186/s12887-021-02507-4
6. Wiysonge, C S, P W Mahasha, D E Ndwandwe, and N J Ngcobo. 2020. “Contextualised strategies to increase childhood and adolescent vaccination coverage in South Africa: a mixed-methods study.” BMJ Open (British Medica Journal) 10(6):e028476. doi:10.1136/bmjopen-2018-028476. Retrieved from https://www.researchgate.net/publication/341936594_Contextualised_strategies_to_increase_childhood_and_adolescent_vaccination_coverage_in_South_Africa_a_mixed-methods_study
2. Center for Disease Control and Prevention. 2019. Pertussis ( Whooping Cough). 25 October. Accessed August 25, 2021. Retrieved from https://www.cdc.gov/pertussis/clinical/features.html.
3. Kandeil, W, E M Bunge, V A Jenkins, M A Ceregido, and A Guignard. 2020. “A systematic review of the burden of pertussis disease in infants and the effectiveness of maternal immunization against pertussis.” Expert Review of Vaccines 19 (7): 621-638. Accessed Aug 28, 2021. doi:https://doi.org/10.1080/14760584.2020.Retrieved from https://www.tandfonline.com/doi/full/10.1080/14760584.2020.1791092?src=recsys
4. Moro, L P, P F Havers, S Hariri, and S Skoff. 2021. Epidemiology and Prevention of Vaccine-Preventable Diseases. Edited by Center for Communicable Diseases. Vol. 14. https://www.cdc.gov/vaccines/pubs/pinkbook/index.html. Accessed August 27, 2021. Retireved from https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/pert.pdf.
5. Wang, C, H Zhang, Y Zhang , L Xu, M Miao, H Yang, Y Liu, S He, and L Pang . 2021. “Analysis of clinical characteristics of severe pertussis in infants and children: a retrospective study.” BMC Pediatrics 21 (Article number: 65 (2021)). Accessed August 27, 2020. doi:https://doi.org/10.1186/s12887-021-02507-4. Retrieved from https://bmcpediatr.biomedcentral.com/articles/10.1186/s12887-021-02507-4
6. Wiysonge, C S, P W Mahasha, D E Ndwandwe, and N J Ngcobo. 2020. “Contextualised strategies to increase childhood and adolescent vaccination coverage in South Africa: a mixed-methods study.” BMJ Open (British Medica Journal) 10(6):e028476. doi:10.1136/bmjopen-2018-028476. Retrieved from https://www.researchgate.net/publication/341936594_Contextualised_strategies_to_increase_childhood_and_adolescent_vaccination_coverage_in_South_Africa_a_mixed-methods_study
Contributor: Linda Ravenhill
Linda Ravenhill is a medical professional with an MA in Journalism. She has worked in the medical, technology and digital development spaces for over 25 years, & has a particular interest in the impact of technology on the delivery of healthcare in the Sub-Saharan Africa region.
Linda Ravenhill is a medical professional with an MA in Journalism. She has worked in the medical, technology and digital development spaces for over 25 years, & has a particular interest in the impact of technology on the delivery of healthcare in the Sub-Saharan Africa region.
Disclaimer
This article is compiled from a variety of resources researched and compiled by the contributor. It is in no way presented as an original work. Every effort has been made to correctly attribute quotes and content. Where possible all information has been independently verified. The Medical Education Network bears no responsibility for any inaccuracies which may occur from the use of third-party sources. If you have any queries regarding this article contact us
Fact-checking Policy
The Medical Education Network makes every effort to review and fact-check the articles used as source material in our summaries and original material. We have strict guidelines in relation to the publications we use as our source data, favouring peer-reviewed research wherever possible. Every effort is made to ensure that the information contained here is an accurate reflection of the original material. Should you find inaccuracies, out of date content or have any additional issues with our articles, please make use of the contact us form to notify us.
Rating
